
Subarachnoid haemorrhage (SAH) can induce vascular smooth muscle contraction within the intracranial arteries which are exposed to the breakdown products of blood within the subarachnoid space. The resultant vasospasm causes a varying degree of arterial narrowing, potentially reducing perfusion to areas of the brain to the extent that ischaemic infarction (stroke) can ensue. Approximately 70% of SAH patients will have vasospasm demonstrable on angiography and 30% will have clinically significant vasospasm.
Routine preventative and therapeutic measures instigated in the Neuro-intensive care unit includes so called "Triple H" therapy consisting of Hypervolaemia, Hypertension and Haemodilution. Intravenous supplementation of magnesium and infusion of a calcium channel blocker (Nimodipine) are also routinely administered at our institution.
In cases of vasospasm refractory to maximal medical management, endovascular treatment may be considered. Balloon angioplasty of the larger arteries at the base of the brain is the preferred treatment and is more durable than chemical angioplasty which involves infusion of verapamil, papaverine or nimodipine directly into the narrowed arterial segments.
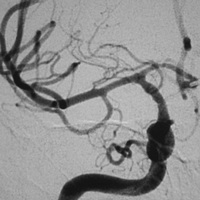 Before treatment |
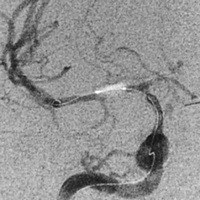 During angioplasty with balloon inflated |
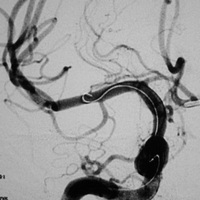 After angioplasty |
 Balloon catheter |
Non-invasive monitoring of the intracranial arteries for the development of vasospasm utilising transcranial doppler (TCD), CT angiography and/or CT perfusion has been employed at some institutions