
A Balloon Test Occlusion (BTO) is used to determine whether sufficient blood flow to the brain can be maintained if one of the major arteries in the neck is intentionally occluded.
The carotid and vertebral arteries are interconnected to varying degrees at the base of the brain. Therefore, occlusion of one or more of these arteries may be tolerated provided the remaining arteries are normal and the interconnections are well developed. Sacrifice or permanent occlusion of one of these arteries is the treatment of choice for some giant aneurysms and fistulas (abnormal artery-to-vein connections). BTO can also provide important information for the neurosurgeon when contemplating the appropriate type of arterial bypass procedure.
BTO is performed with the patient awake to permit assessment of neurological status. A balloon is temporarily inflated in the neck to occlude the artery being tested during which time the patient is continually monitored and examined for the development of any weakness, speech disturbance, and so on. Adjunctive electroencephalography (EEG) monitoring and formal testing by a neuropsychologist is sometimes utilised. If no change in neurological status is evident after 15 minutes of testing, a hypotensive challenge may be initiated during which the patient’s blood pressure is gradually reduced by 20-25% of baseline with the help of our anaesthetic colleagues. Passing a BTO including this manoeuvre increases our confidence that the artery can be safely sacrificed. After 30 minutes of testing or as soon as a neurological deterioration is detected, the balloon is deflated and blood flow re-established.
Due to blood flow stasis downstream from the point of occlusion by the balloon in the artery being tested, we routinely administer an anticoagulant (heparin) to minimise the risk of clot formation. Patients should ideally be premedicated with aspirin before the procedure for its anti-platelet effect.
Permanent vessel occlusion / sacrifice may be performed at the same sitting after passing a BTO in some cases. This is usually achieved using detachable balloons and/or metal coils. The patient is subsequently nursed strictly supine overnight in the Neuro-intensive care unit and maintained on aspirin for 2 weeks.
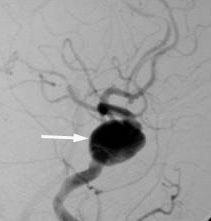 Giant cavernous internal carotid artery (ICA) aneurysm |
The patient passed a BTO and the ICA was subsequently occluded with balloons at the same sitting |
